Sweet syndrome (SS) - acute febrile neutrophilic dermatosis - is an uncommon inflammatory disorder characterized by the abrupt appearance of painful, edematous, and erythematous papules, plaques, or nodules on the skin. Fever and leukocytosis frequently accompany the cutaneous lesions. 13 SS presents in three clinical settings: classical, malignancy-associated and drug-induced. 4 Mycobacterium tuberculosis (MT) showing SS is an extremely uncommon association. 5,6
A 61-year-old female presented to the emergency department with a 3-day history of fever and multiple well-circumscribed erythematous-to-violaceous papules and plaques with vesicular borders, distributed in an asymmetrical fashion over her head, chest, back, and limbs (Fig. 1). The patient reported no other symptoms. She was diagnosed with rickettsia infection, prescribedd doxycycline and discharged home. In a revision appointment, she presented poor outcome and was admitted in an internal medicine ward.
Fig 1:Edematous erythematous papules and plaques in the legs (A and B). Well-demarcated erythematous papules with centrifugal extension in the arm (C).
Only then she reported recent weight loss. Blood tests revealed the persistence of inflammatory parameters. Biopsy of the skin lesions demonstrated a diffuse neutrophilic dermatosis - SS was established and the patient treated with prednisone.
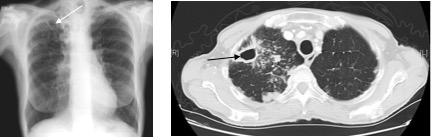
Chest X-ray and CT-scan disclosed a diffuse micronodular infiltrate in both lungs and a parenchyma densification in the right upper lobe suggestive of pulmonary tuberculosis (Fig.2). Sputum smear and culture were positive for MT so the patient started anti-tuberculosis standard three-drug regimen.
Fig 2. A Chest X-ray Multifocal patchy opacities in the right upper lobe (white arrow). B - The Chest CT scan demonstrates the thick walled cavity in the anterior segment of the right upper lung (black arrowed).
SS is considered to be a skin manifestation of a systemic disease and in this case was the presentation symptom of pulmonary tuberculosis.
Figura I

Edematous erythematous papules and plaques in the legs (A and B). Well-demarcated erythematous papules with centrifugal extension in the arm (C).
Figura II
Chest X-ray Multifocal patchy opacities in the right upper lobe (white arrow). B - The Chest CT scan demonstrates the thick walled cavity in the anterior segment of the right upper lung (black arrowed).
BIBLIOGRAFIA
1. Sweer RB. an acute febrile neutrophilic dermatosts. Br J Dermatol [Internet]. 1964 Aug 1 [cited 2017 Dec 31];76(89):34956. Available from: http://doi.wiley.com/10.1111/j.1365-2133.1964.tb14541.x
2. Su WP, Liu HN. Diagnostic criteria for Sweets syndrome. Cutis [Internet]. 1986 Mar [cited 2017 Dec 31];37(3):16774. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3514153
3. Geller BJ, Stone RM, Merola JF, Levy BD, Loscalzo J. A Man with Fever, Cough, and Rash. Solomon CG, editor. N Engl J Med [Internet]. 2015 Jul 2 [cited 2017 Dec 14];373(1):7480. Available from: http://www.nejm.org/doi/10.1056/NEJMcps1404270
4. Cohen PR. Sweets syndrome--a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis [Internet]. 2007;2:34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17655751%5Cnhttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC1963326
5. Mrabet D, Saadi F, Zaraa I, Chelly I, Sahli H, Osmane AB, et al. Sweets syndrome in a patient with rheumatoid arthritis, Sjogrens syndrome and lymph node tuberculosis. Case Reports [Internet]. 2011 Feb 2;2011(jan29 1):bcr0720103137-bcr0720103137. Available from: http://casereports.bmj.com/cgi/doi/10.1136/bcr.07.2010.3137
6. Ledoult E, Becquart C, Chanson N, Sobanski V, Remy-Jardin M, Delaporte E, et al. Sweet syndrome and disseminated Mycobacterium tuberculosis infection. Eur J Dermatology [Internet]. 2016 Jan 1 [cited 2017 Dec 14];26(1):99100. Available from: http://www.jle.com/fr/revues/ejd/e-docs/sweet_syndrome_and_disseminated_mycobacterium_tuberculosis_infection_306446/article.phtml

