A 68-year-old male smoker presented with acute lower respiratory infection and a two-month history of right hemiparesis and aphasia with no previous etiologic investigation. The neurologic examination revealed obtundation, global aphasia and right spastic hemiparesis. A cerebral computerized tomography (CT) revealed multiple bilateral axial lesions with central loss and margin gain of density, cerebral edema, mass effect on the left lateral ventricle and deviation from the midline to the right (figure 1). Blood and sputum cultures, as well as serologic tests for HIV, syphilis, Toxoplasma, Cryptococus and Toxocara were negative. Given the patients symptoms and signs of increased intracranial pressure, no attempt at a lumbar puncture was made. Magnetic resonance imaging (MRI) of the brain revealed multiple bilateral cystic lesions with margin hyperintensity on T2 Flair, without diffusion restriction, suggesting a neoformation (figure 2). A chest CT revealed multiple mediastinic and hilar adenopathies and a 3cm solitary pulmonary nodule on the pulmonary medium right lobule, suggestive of a primary proliferative lesion. Despite resolution of the initial respiratory infection, worsening dysphagia and increased risk of aspiration ensued. There was no response to corticosteroid therapy for cerebral edema, probably because of the predominance of the mass effect. Given the patients functional status and advanced disease, no further diagnostic or therapeutic measures were taken beyond symptomatic control. The patient died 2 weeks later from respiratory infection.
Cystic brain lesions are unusual1 and remain a diagnostic challenge because of nonspecific clinical and radiological findings2. Cerebral metastases should be considered in the differential diagnosis. Although loss of signal in T1 and increased signal in T2-weighted MRI images are shared characteristics of both infectious and metastatic cystic lesions3, absence of diffusion restriction in MRI diffusion-weighted sequences is highly suggestive of metastization, and its use helpful in leading to a prompt treatment3.
CONFLICT OF INTERESTS:
Nothing to declare.
FINANCING SOURCE:
None to declare.
Figura I
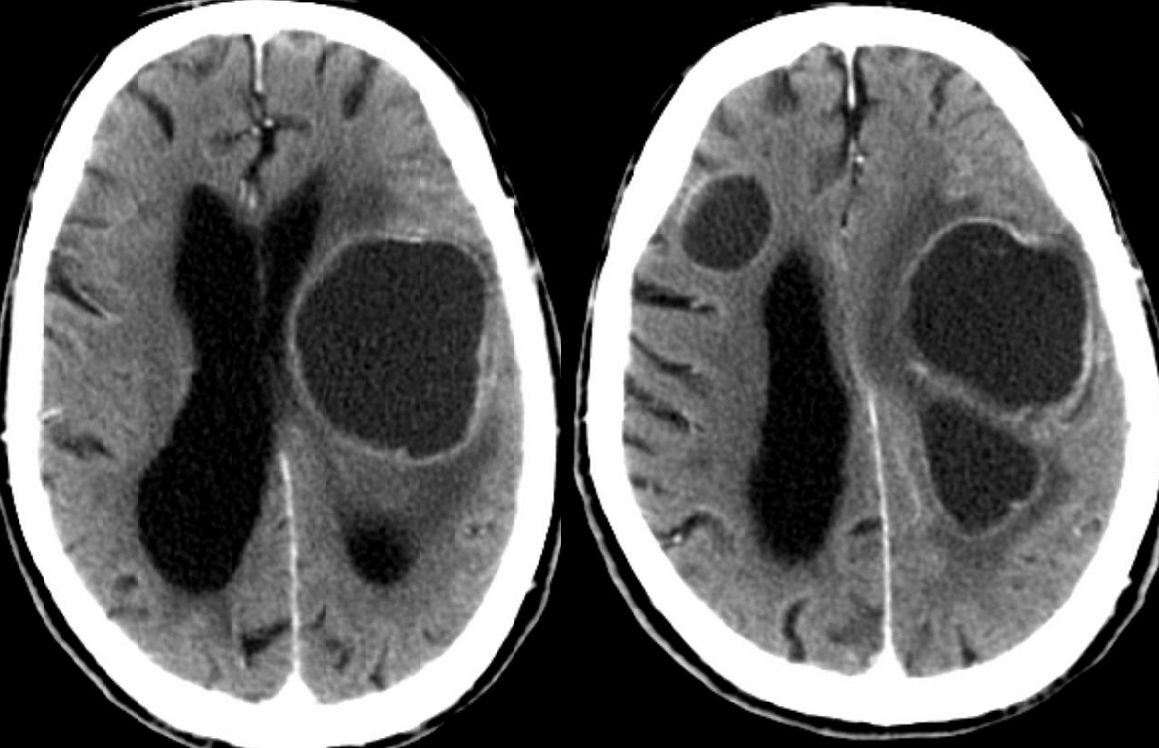
Multiple intracoronial cortico-subcortical lesions, with a cystic configuration, defining peripheral halo isodense with the cortex that undergoes strong enhancement after contrast and central hypodensity. Mass effect is associated with ventricular system casting.
Figura II
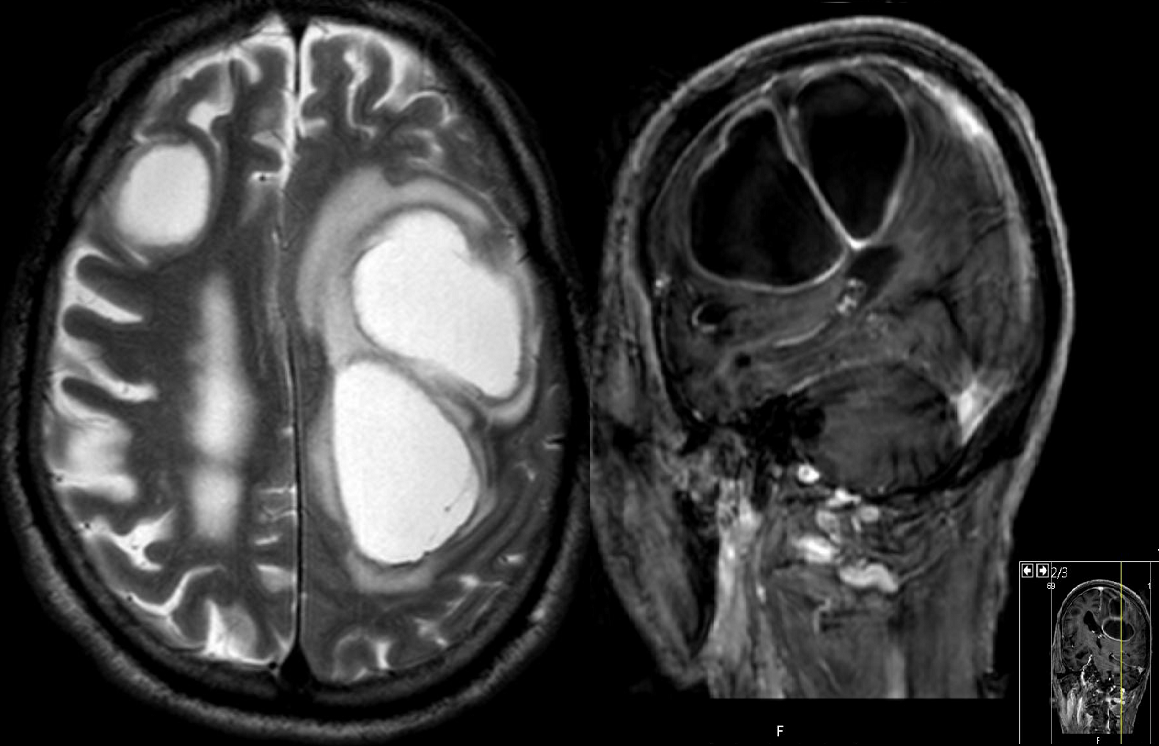
The lesions exhibit central hypersignal in T2, with decanted contents in the posterior region with low signal in T2 and T2 * of possible hematic or necrotic nature. Peripheral uptake is found and vasogenic edema of the encircling brain parenchyma is observed. No foci of restriction to the diffusion of water molecules are observed. Brain atrophy coexists.
BIBLIOGRAFIA
1. Alexey Surov, Michael Hainz, Malte Kornhuber. Multiple Cystic Metastases in the Brain from Adenocarcinoma of the Lung. The American Journal of Medicine. 2009. 122;
2.Young Jun Kim, Kee-Hyun Chang, In Chan Song, Hong Dae Kim, Su Ok Seong, Young Hoon Kim et al. Brain Abscess and Necrotic or Cystic Brain Tumor: Discrimination with Signal Intensity on Diffusion Weighted MR Imaging. ARJ. 1998. 171: 1487-1490;
3.Alexandra Oprisan and Bogdan O. Popescu. Intracranial Cysts: An Imagery Diagnosis Challenge. The Scientific World Journal. 2013.

