Doente do sexo masculino, de 75 anos, com história de cirurgia hepática por motivo desconhecido é admitido no serviço de urgência por quadro com duas semanas de evolução de dor abdominal intermitente e oligoanúria. À palpação abdominal apresentava volumosa massa abdominal dolorosa que se estendia do epigastro ao hipogastro. Realizou ecografia abdominal, tomografia computorizada (Fig. 1A e 1B) e ressonância magnética que mostraram gigante quisto de 28x19x18cm, que se estendia do fígado até à cavidade pélvica, causando ureterohidronefrose, com aparência de rosário pela presença de múltiplas vesículas filhas (seta pequena), sugerindo o diagnóstico de quisto hidático (seta grande). A serologia foi positiva para Ac anti-Echinococcus (titulo de 1:512), tendo realizado um ciclo de 28 dias de albendazol. Após terminar o anti-parasitário foi submetido a excisão radical do quisto (Fig. 2A e 2B), o diagnóstico definitivo foi confirmado por exame anatomopatológico e teve alta clinicamente melhorado. A Equinococcose, ou doença hidática, é uma zoonose causada pela larva do géneroEchinococcus1 e o fígado é a localização mais frequente de quistos2. O seu crescimento é associado a resposta imune do hospedeiro com o desenvolvimento de um camada fibrosa, septações e vesículas filhas no interior do quisto primário1. O diagnóstico pode ser incidental, uma vez que a doença pode ser assintomática, no entanto, é sabido que os quistos crescem, em media, um centímetrode diâmetro nos primeiros 6 meses, e depois 2-3cm por ano3. Assim, os quistos hidáticos gigantes são raríssimos, pelo aumento considerávelde sintomas e complicações potencialmente fatais à medida que aumentam detamanho4. Uma vez estabelecido o diagnóstico, quatro modalidades terapêuticas estão disponíveis: antibioterapia, cirurgia (por via aberta ou via laparoscopica), drenagem percutânea ou vigilância clínica2,5. Hoje em dia, a abordagem recomendada deve ter em conta as características clínicas e imagiologicas do doente6.
A 75-year-old man, with previous hepatic surgery of unknown etiology, was admitted with a 2-weeks history of intermittent abdominal discomfort and oligoanuria. Physical examination revealed a painful abdominal mass, extending from the upper to the lower quadrants of the abdomen. Ultrasounds, abdomino-pelvic compute tomography (Fig. 1A and 1B) and magnetic resonance were performed, showing a large cystic mass measuring 28x19x18cm, involving the liver and pelvic cavity, compressing the bladder, causing ureterohydronephrosis, with rosary appearance due to multiple daughter cysts (small arrow), suggesting the diagnosis of hydatid cyst (large arrow). Serologic testing was positive for Echinococcosis (titer 1:512) and a 28 days cycle of anti-parasitic therapy with albendazole was performed. Afterwards, the patient underwent surgery and radical excision was performed (Fig. 2A and 2B). The diagnosis was confirmed by anatomical examination and the patient was discharged after complete recovery. Echinococcosis, or hydatid disease, is a zoonosis caused by the larval stages ofTaeniacestodes belonging to the genusEchinococcus1 andthe liver is the most frequent location for parasitic cysts2. Cyst expansion is associated with a host immune reaction and the development of a fibrous layer and old cysts typically present internal septations and daughter cysts1. As its course is usually asymptomatic, the diagnosis may often be incidental, but it has been reported that hepatic hydatid cysts grow one centimeter in diameter during the first six months and then two to three centimeters annually; this is strictly related to the surrounding tissue resistance3. Giant hydatid cysts are extremely rare once as the cyst grows, symptoms and complications become more common and can be severe4. Once the diagnosis is established, the therapeutic approach to treat hepatic Echinococcosis include chemotherapy, surgery (open or laparoscopic), percutaneous treatments and watch and wait strategy2,5. Nowadays, a stage-specific approach is recommended, according to the disease characteristics6.
Figura I
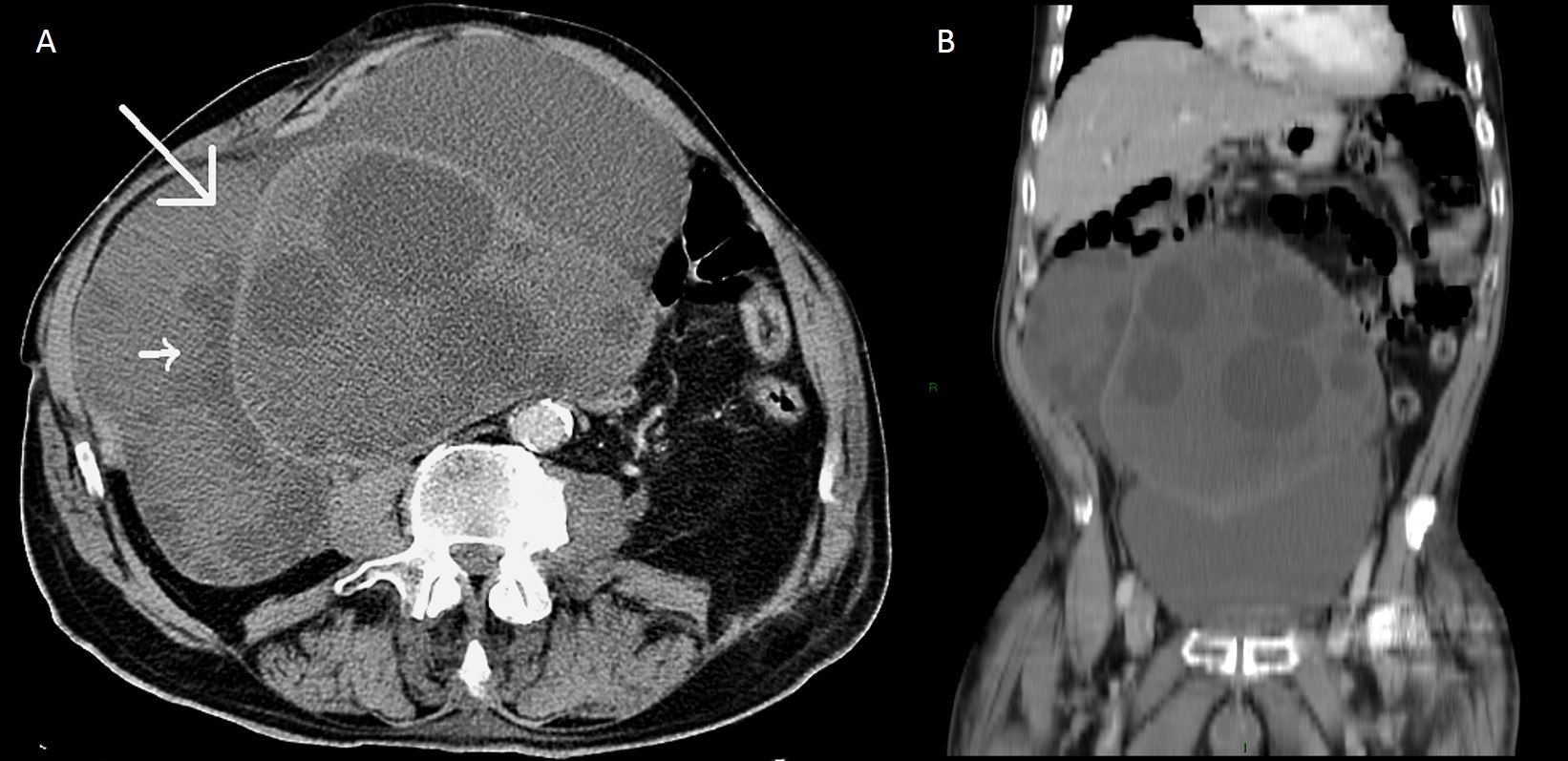
A: TC axial após administração de contraste IV em fase portal. Vesiculas filhas hipoatenuadas com vesícula mãe ligeiramente hiperatenuada; B: TC coronal que evidencia o volumoso quisto - vesícula mãe ligeiramente hiperatenuada e vesiculas filhas hipoatenuadas
Figura II
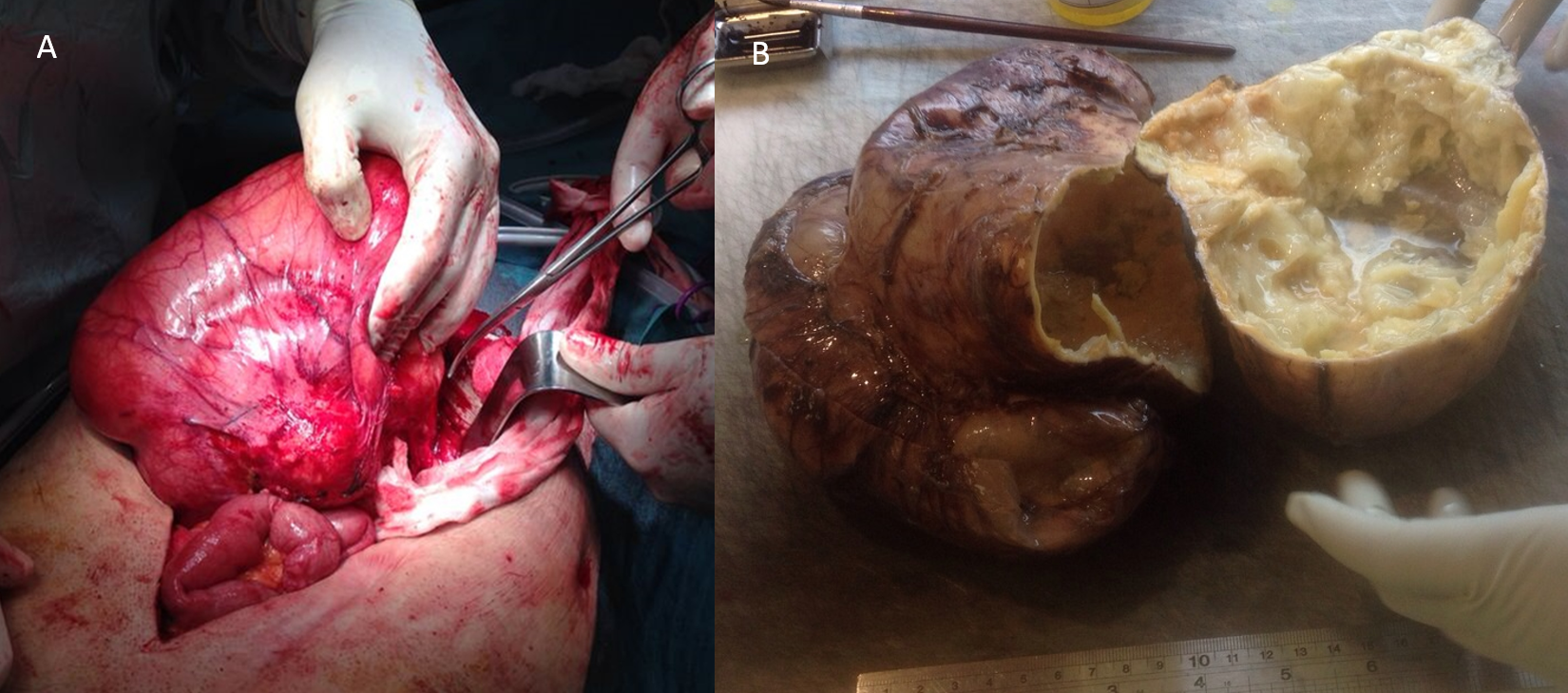
A: Quisto hidático (intra-operatório); B: Interior do quisto hidático
BIBLIOGRAFIA
1. Giuseppe Nunnari, Marilia R Pinzone, et al; Hepatic echinococcosis: Clinical and therapeutic aspects; World J Gastroenterol.2012 April 7;18(13): 14481458.
2. Francesca Rinaldi, Enrico Brunetti, et al; Cystic echinococcosis of the liver: A primer for hepatologists; World J Hepatol. 2014 May 27; 6(5): 293305.
3. Aydin U, Yazici P, Onen Z, Ozsoy M, Zeytunlu M, Kiliç M, Coker A. The optimal treatment of hydatid cyst of the liver: radical surgery with a significant reduced risk of recurrence.Turkish J Gastroenterology.2008;19:3339.
4.Sahin DA, Kusaslan R, Onder S, Dilek ON. Huge hydatid cysts that arise from the liver, growing exophytically.Can J Surg.2007;50:301303.
5. Brunetti E, Kern P, Vuitton DA. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans.Acta Trop.2010; 114:116.
6.Srinivas MR, Deepashri B, Lakshmeesha MT. Imaging Spectrum of Hydatid Disease: Usual and Unusual Locations.Polish Journal of Radiology. 2016;81:190-205.

