A woman, 86 years old, presented to the emergency department with fatigue, anorexia, nausea and vomiting. She had history of anemia, recurrent urinary tract infections (UTI) and staghorn calculi (StC) (figure 1-A). The physical examination was unremarkable. Blood analysis revealed: Hemoglobin 9,4 g/dL; 14000 leucocytes/mcL with 81,5% neutrophils and reactive C-protein 14,4 mg/dL. Urinalysis revealed leucocytes, hemoglobin and identified Proteus mirabilis. Cefuroxime was started for uncomplicated cystitis. Despite adequate antibiotic treatment, her clinical condition deteriorated. Another urine culture was obtained and piperacilin/tazobactan initiated. An abdominal CT scan identified a big StC and an abscess in the superior pole of the right kidney connected with another in the liver (figure 1-B), suggesting xanthogranulomatous pyelonephritis (XP) with hepato-renal abscess. CT guided drainage was performed and additional 40 days of antibiotic made before total nephrectomy. Few days after surgery, the patient died in the intensive care unit. The histologic exam revealed squamous cell carcinoma (SCC) of the renal pelvis with local infection.
XP is an uncommon type of chronic pyelonephritis. Occurs more frequently in middle aged women with predisposing factors: recurrent UTI, renal calculi formation (mainly StC), chronic urinary tract obstruction, abnormal lipid metabolism and immunological anomalies. It destroys the renal parenchyma and peri-renal tissues making it difficult to distinguish from other entities. The CT is the gold standard diagnostic exam, though only histologic exam confirms it. Although antibiotic therapy can be done, only radical nephrectomy solves this condition.1
Unexpectedly, in this patient another entity lead to the fatal outcome. SCC of the renal pelvis is rare (0,5-15% of urothelial malignancies) and, similarly to XP, is associated with chronic lithiasic obstruction and chronic UTI with parenchymal atrophy.2 Clinical and radiologic findings are not specific so the diagnosis is frequently made late in the course of the disease, thus overshadowing the prognosis.3
Figura I
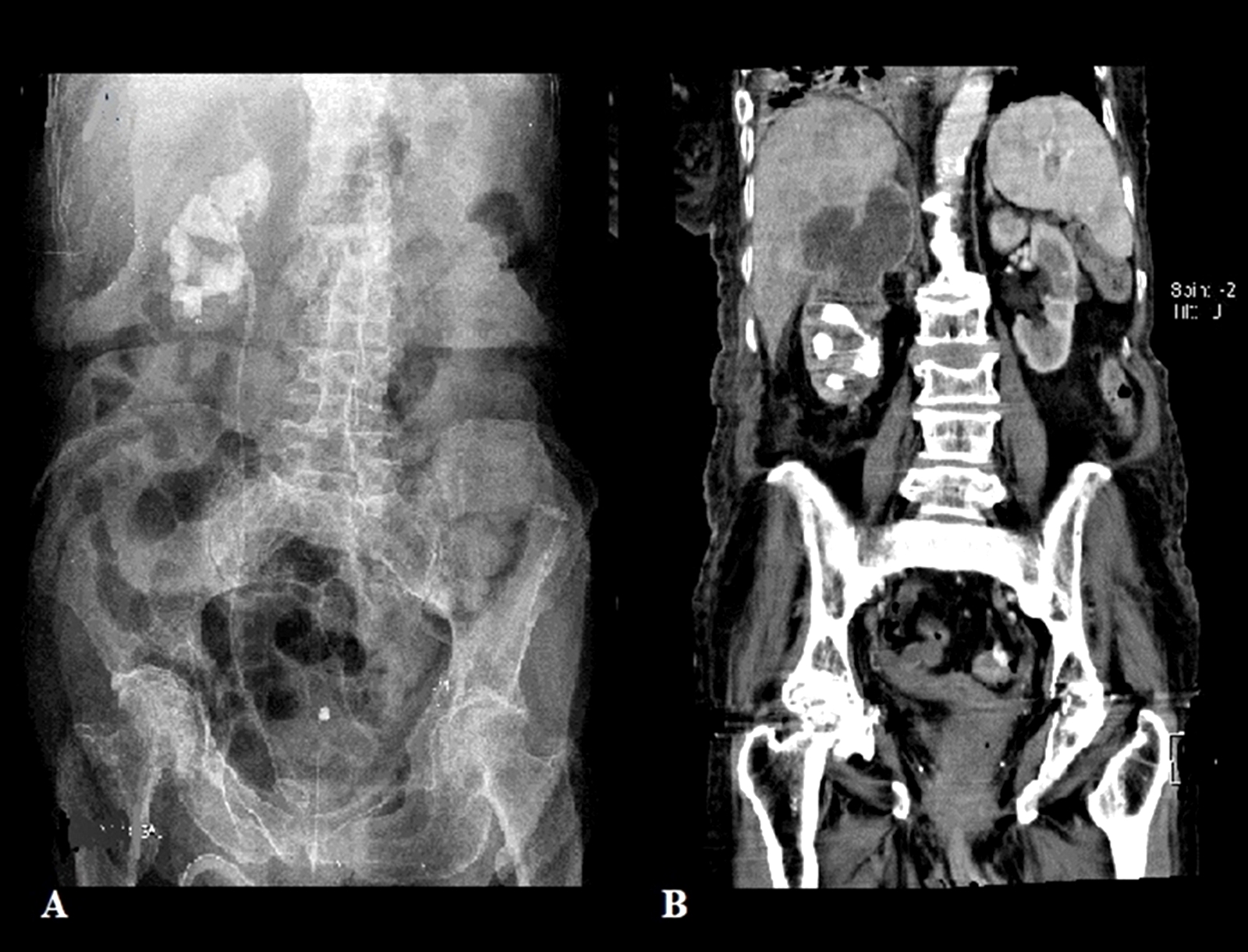
A) Large staghorn calculi in the abdominal X-ray ; B) Abdominal CT scan with big staghorn calculi in the right kidney and an abscess in the superior pole connected with another in the liver.
BIBLIOGRAFIA
1. Siddappa, S. et al- Xanthogranulomatous Pyelonephritis: A Retrospective Review of 16 Cases. Korean Journal of Urology. 2011; 52:421-424.
2. Jongyotha, K; Sriphrapradang, C. - Squamous Cell Carcinoma of the Renal Pelvis as a Result of Long-Standing Staghorn Calculi. Case Reports Oncology 2015;8:399404
3. Attalla, K. et al - Squamous Cell Carcinoma of the Renal Pelvis: Atypical Presentation of a Rare Malignancy. Urology Case Reports. 2017; 137 -139.

