Introduction: Porto-sinusoidal vascular liver disease (PSVD) is defined by the occurrence of portal hypertension in the absence of portal vein thrombosis and cirrhosis, with mild or moderate alterations of liver histology.1
This new entity encompasses a heterogeneous group of vascular liver diseases previous described, namely idiopathic non-cirrhotic portal hypertension or nodular regenerative hyperplasia.2,3
PSVD has multiple etiologies such as immunologic, blood and genetic diseases, prothrombotic conditions and drugs. Oxaliplatin is one of the most common associated chemotherapy agents, described in until 15% of patients.4,5
Clinical case: We present a case of a 60-year old man, without previous history of liver disease, submitted in April 2012 to a total gastrectomy due to a signet-ring cell gastric cancer (pT1N1M0), followed by 6 cycles of adjuvant chemotherapy with EOX regimen (epirubicin, oxaliplatine and capecitabine) and surveillance.
Patient was asymptomatic until January 2017 when he was admitted with acute esophageal variceal bleeding. Abdominal CT scan showed patency of portal vein, perihepatic ascites and nodular configuration of segment III (Fig. 1). Tumor markers were normal and common causes of cirrhosis were excluded. Median liver stiffness on elastography was 10.1 kPa and hepatic venous pressure gradient was 4 mmHg. A liver biopsy of segment III and of the right lobe was performed which excluded cirrhosis or neoplastic involvement (Fig. 2). Diagnosis of PSVD due to oxaliplatin was made.
Conclusion: In patients treated with oxaliplatin in the presence of clinical signs of portal hypertension, the diagnosis of vascular liver disease should be considered. Findings can mimick liver neoplastic involvement as described in our case report. In this population biopsy should be pursued to exclude the diagnosis of malignancy and avoid overtreatment. The natural history of PSVD is not yet fully known but patients require screening for portal vein thrombosis and management of portal hypertension complications.
Figura I
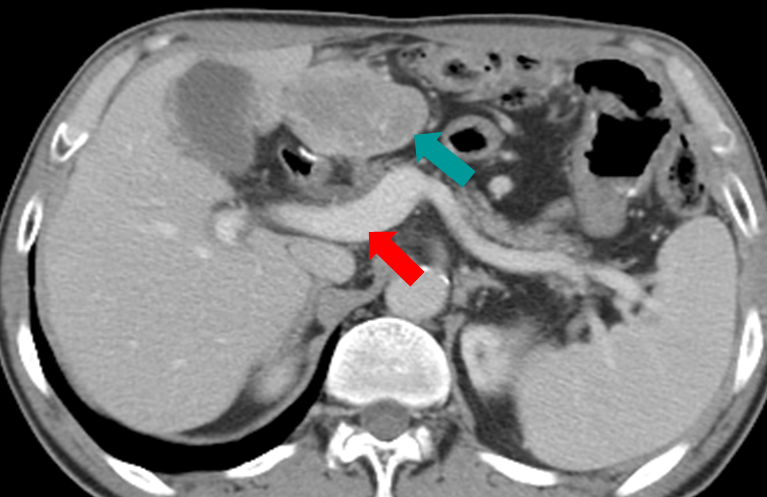
CT scan in transverse section with venous phase contrast showing patency of portal vein (red arrow) and nodular configuration of segment III (blue arrow), without features of cirrhosis and with small perihepatic ascites.
Figura II
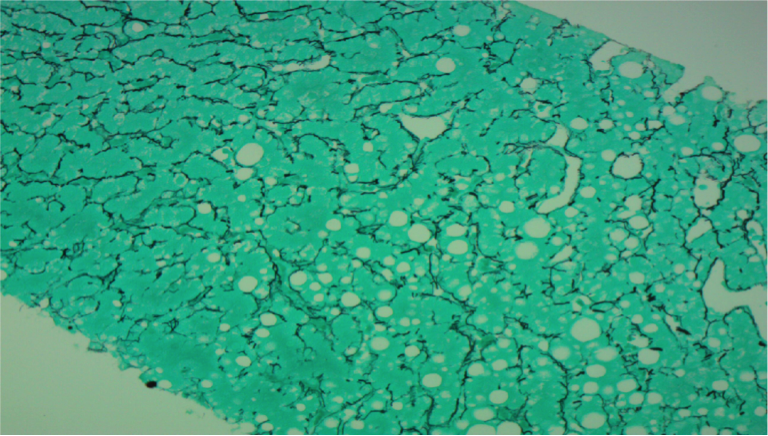
Liver histology reticulin stain (200x) without fibrous septa, with discrete signs of regeneration without nodules, with steatosis without steatohepatitis.
BIBLIOGRAFIA
1. De Gottardi A, Rautou P-E, Schouten J, Rubbia-Brandt L, Leebeek F, Trebicka J, et al. Porto-sinusoidal vascular disease: proposal and description of a novel entity. Lancet Gastroenterol Hepatol. 2019 May;4(5):399411.
2. Schouten JNL, Garcia-Pagan JC, Valla DC, Janssen HLA. Idiopathic noncirrhotic portal hypertension. Hepatology. 2011 Sep 2;54(3):107181.
3. Barge S, Grando V, Nault J-C, Broudin C, Beaugrand M, Ganne-Carrié N, et al. Prevalence and clinical significance of nodular regenerative hyperplasia in liver biopsies. Liver Int. 2016 Jul;36(7):105966.
4. Rubbia-Brandt L, Audard V, Sartoretti P, Roth AD, Brezault C, Le Charpentier M, et al. Severe hepatic sinusoidal obstruction associated with oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Ann Oncol Off J Eur Soc Med Oncol. 2004 Mar;15(3):4606.
5. Slade JH, Alattar ML, Fogelman DR, Overman MJ, Agarwal A, Maru DM, et al. Portal Hypertension Associated With Oxaliplatin Administration: Clinical Manifestations of Hepatic Sinusoidal Injury. Clin Colorectal Cancer. 2009 Oct;8(4):22530.

