A previously healthy 42-year-old caucasian woman, with a smoking history, presented with constitutional symptoms, fever, postprandial abdominal pain and high blood pressure significantly different between both upper limbs. The laboratory tests showed anaemia of chronic inflammation, elevated erythrocyte sedimentation rate (ESR) and C reactive protein levels. The other blood test results were unremarkable. Large vessel arteritis was the most likely aetiogical diagnosis, confirmed by whole-body PET scan that showed increased 18F-FDG uptake of the ascending aorta, in the aortic arch and descending aorta. Gadolinium-enhanced magnetic resonance angiography revealed a bilateral occlusion of the internal carotid arteries (Fig. 1). Classic angiography showed an occlusion of the celiac trunk and superior mesenteric artery (Fig. 2), with a network of collateral circulation. Immunosuppressive therapy with prednisolone and metothrexate was initiated, with normalization of ESR and improvement of abdominal pain and reduction of 18F-FDG uptake within one month of treatment.
Takayasu arteritis is an idiopathic chronic large-vessel vasculitis that presents with symptoms related to end-organ ischemia, involving more frequently the aorta and its proximal branches.
1 Most patients have at least mild cervical vascular disease, but cervical internal carotid artery involvement is rare.
2 This diseases slow progression can result in severe panarterial stenoses and/or occlusions with mild or no symptoms of end-organ ischemia, due to the development of collateral circulation. Diagnosis can be made on clinical findings in the setting of compatible vascular imaging abnormalities, according to the American College of Rheumatology criteria.
3 The NIH criteria assesses disease activity through constellation of clinical, ESR and serial imaging and more recently ITAS2010 and ITAS-A have been also validated to measure disease activity.
4 Glucocorticoids are the mainstay for initial therapy, however, an additionally immunosuppressive agent is required in most cases to ensure disease remission.
5 Surgical or endovascular intervention, if necessary, for chronic end-organ ischemia or aneurysmal degeneration, is ideally delayed until the disease is quiescent.
5Figura I

Figure 1: gadolinium-enhanced magnetic resonance angiography shows bilateral occlusion of the internal carotids in a coronal view (blue arrows) and in an oblique view (red arrows). Segmental narrowing of the right subclavian artery is showed by the yellow arrow.
Figura II
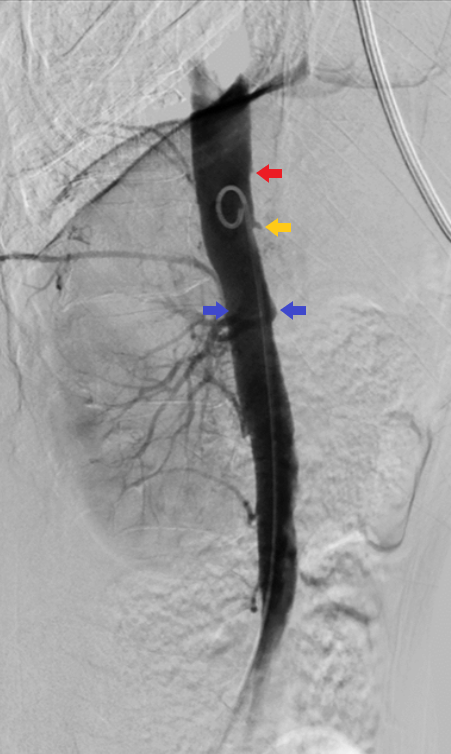
Figure 2: Angiography, lateral view, showing occlusion near the origin of celiac trunk and superior mesenteric artery (red and yellow arrows). The blue arrows show the origin of the renal arteries.
BIBLIOGRAFIA
1 - Onen F, Akkoc N. Epidemiology of Takayasu arteritis.Presse Med. 2017; 46 (7-8 Pt2):e197-e203.
2 - Bond KM, Nasr D, Lehman V, Lanzino G, Cloft HJ, Brinjikji. Intracranial and Extracranial Neurovascular Manifestations of Takayasu Arteritis. AJNR Am J Neuroradiol. 2017; 38(4):766-72.
3 -Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, et al. The American College of Rheumatology criteria for the classification and Takayasu arteritis.Arthritis Rheum 1990; 33(8):1129-34.
4 - Misra DP, Misra R. Assessment of disease activity in Takayasu´s arteritis. Indian J Rheumatol. 2015; 10(5):43-7.
5 - Maksimowicz-McKinnon K, Hoffman GS. Takayasu arteritis: What is the long-term prognosis?Rheum Dis Clin North Am. 2007; 33(4):777-86.

