The authors present the report of a 24 year-old immunocompetent man observed in the Emergency Department with a history of sudden onset of generalized myalgia followed by painful lesions on the palm of hands, soles of feet and oral mucosa over the last 48h. There were no other systemic complaints. He was otherwise healthy, with no contact with children of any age The lesions were non-pruritic, painful when compressed, diameter ranging from 1-2 mm, with a visible erythematosus halo; the ones in the palm of the hands and feet were 5 to 10 in number and the ones in the oral mucosa, distributed along the hard palate and in the gum, were scarce and softer (Figure 1 a,b and c.). The remaining clinical examination failed to reveal any abnormality, most specifically there was no organ size anomaly or palpable lymph nodes. Blood work-up revealed a normal erythrocyte and platelet count, with no leukocytosis (5.72x109/L), normal differential with neutrophil and lymphocyte absolute counts of 2800 and 2000, respectively and normal biochemistry. Coxsackie A16 IgM antibodies were reactive, IgG negative.
The clinical suspicion of Hand-Feet-Mouth Syndrome (HFMS) was high in this patient, even lacking epidemiological history. The lesions were very suggestive considering their localization and characteristics; the confirmation was provided with the antibody positivity for the Coxsackie A16 virus. The patient underwent nonsteroidal anti-inflammatory treatment, with complete regression of the lesions (Figure 2.a,b,c) in a one week span of diclofenac 75mg 2tid and hydration. He was observed in consultation a week later, asymptomatic and with no dermatological complaints.
HFMS is a very sporadic diagnostic in the adult patient. The majority of the cases described in adults mimic the pediatric syndrome,1 rarely presenting with atypical symptoms.2 Considering the typical cases described, most of the subjects had had contact with sick children suffering from HFMS, which eased the degree of suspicion. HFMS is caused by Coxsackie serotypes from A1 to 6,8,10 and 223; the serotype involved is also important to consider: our patient suffered a very mild syndrome, typically caused by the A16 serotype. As to the aspect of the lesions, our patient did not have ulcerative lesions nor were those fit to sample. The serological diagnosis is preferable to lesion sampling and fluid molecular testing, the latter unavailable in most centers, as in our case.
The differential diagnosis of HFMS in adults includes conditions associated with oral lesions,4,5 that would include herpangina, aphthous ulcers and primary herpes simplex gingivostomatitis.
In conclusion, despite being an infrequent diagnosis, HFMS in adults may occur and it is important to bear in mind the hallmarks that define this viral syndrome to recognize it easily, since it is a very benign, treatable condition. The management is focused in supportive treatment and complications are rare.6Making the correct diagnostic may be challenging, namely if the patient is observed in the urgency department.
Figura I
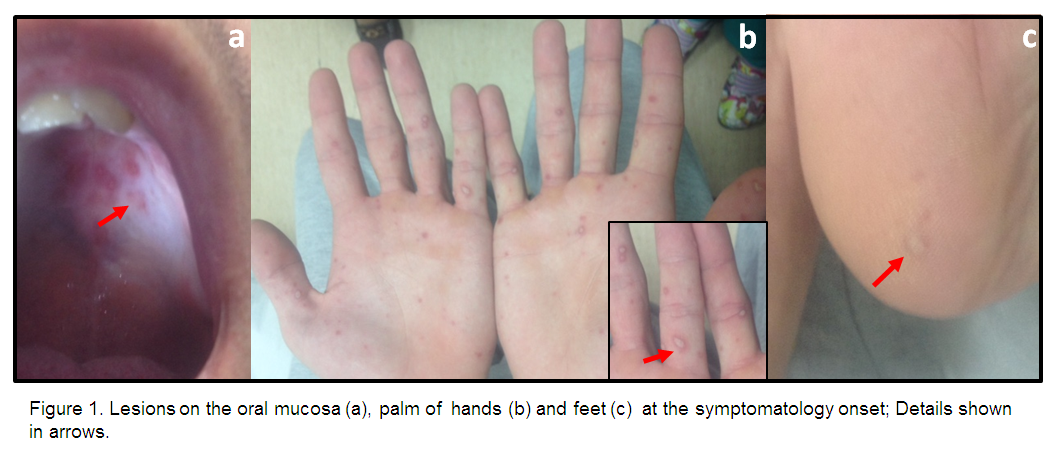
Lesions in the oral mucosa (a), palm of hands (b) and feet (c), at the symptomatology onset. Details shown in arrows.
Figura II
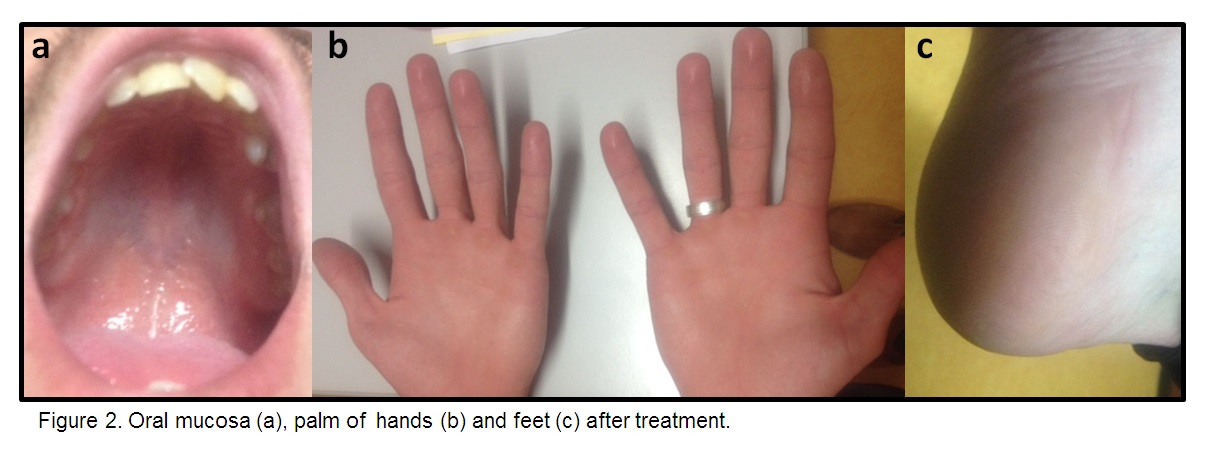
Oral mucosa (a), palm of hands (b), and feet (c) after treatment.
BIBLIOGRAFIA
References:
1. Ślebioda Z,Dorocka-Bobkowska B. Hand, foot and mouth disease as an emerging public health problem: Case report of familial child-to-adult transmission.Dent Med Probl.2018 Jan-Mar;55(1):99-104. doi: 10.17219/dmp/80995.
2. Ben-Chetrit E,Wiener-Well Y,Shulman LM,Cohen MJ,Elinav H,Sofer D,Feldman I,Marva E,Wolf DG. Coxsackievirus A6-related hand foot and mouth disease: skin manifestations in a cluster of adult patients. J Clin Virol.2014 Mar;59(3):201-3. doi: 10.1016/j.jcv.2013.12.012.
3. Park K, Lee B, Baek K, Cheon D, Yeo S, Park J, Soh J, Cheon H, Yoon K, Choi Y.Enteroviruses isolated from herpangina and hand-foot-and-mouth disease in Korean children. Virol J. 2012;9:205. doi: 10.1186/1743-422X-9-205.
4. Horsten HH,Kemp M,Fischer TK,Lindahl KH,Bygum A. Atypical Hand, Foot, and Mouth Disease Caused by Coxsackievirus A6 in Denmark: A Diagnostic Mimicker. Acta Derm Venereol.2018 Mar 13;98(3):350-354. doi: 10.2340/00015555-2853
5. Uptodate.https://www.uptodate.com/contents/hand-foot-and-mouth-disease-and-herpangina search=hand%20foot%20and%20mouth%20disease&source=search_result&selectedTitle=1~23&usage_type=default&display_rank=1;2018 [assessed the 3rd January 2020].
6. Ventarola Daniel, Bordone Lindsey, Silverberg Nanette, Update on Hand Foot Mouth Disease. Clinics in Dermatology (2014). doi: 10.1016/j.clindermatol.2014.12.011.

