A healthy, 40-year-old female, with breast implants, went to the Emergency Ward, presenting oppressive and intermittent postprandial epigastric pain, with 3-week evolution (denied other constitutional symptoms or complaints). Physical examination was unremarkable, but the abdominal X-ray showed osteoblastic lesions in the pelvis (Fig. 1). Consequently, the patient was submitted to a thoraco-abdominopelvic tomography (Fig. 2) that showed lesions sugestive of diffuse metastasis without evidence of a primary lesion or other foci of metastasis. The complementary studies, to help defining primary neoplasia, revealed no changes. For aetiological clarification of the bone lesions a bone biopsy was performed suggesting osteopoikilosis, as well as a bone scintigraphy that showed no fixation foci suggestive of metastasis. However, a breast resonance, due to breast implants, was performed which surprisingly revealed a mammary nodule with an anatomopathological examination compatible with invasive lobular carcinoma.
Osteopoikilosis is a benign and rare autosomal dominant osteosclerotic dysplasia, without prevalence of sex.1,2 At presentation, patients are usually asymptomatic, and lesion are often an incidental finding.3 Well-defined sclerotic lesions clustered symmetrically around joints and throughout the appendicular skeleton and pelvis.2 A differential diagnosis should be considered, especially against osteoblastic metastasis, which present high scintigraphic activity.2-4
In the described case, there were lesions in the spine, which according to the literature arent typical, which led to an exhaustive investigation in search of its etiology, more specifically a primary neoplasm.1-4 Including the performance of bone biopsy and scintigraphy, that proved to be lesions compatible with Osteopoikilosis. Coincidentally the patient had a breast-cancer that was eventually diagnosed.
Despite being benign lesions and is not necessary follow-up or another studies and treatment none required, an early recognition is essential to prevent unnecessary emotional distress.5 In this case, the whole investigation became beneficial for the patient, with the diagnosis of breast-cancer at a still asymptomatic stage.
Figura I
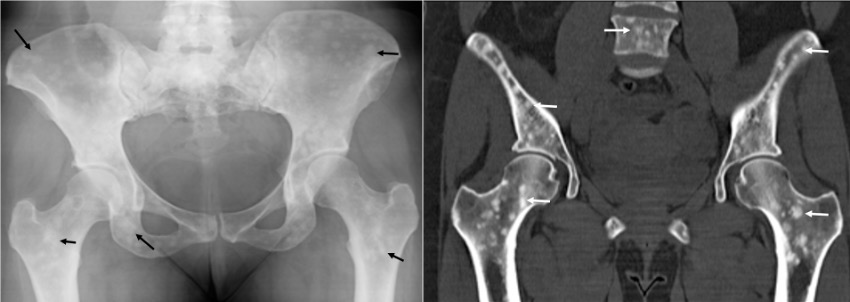
Left on Figure 1 a Pelvic X-ray and Right on Figure 2 a Abdominopelvic tomography showing osteoblastic lesions.
BIBLIOGRAFIA
1. Stephen Wallace; Richard B. Towbin; and Alexander J. Towbin. Osteopoikilosis. APPLIED RADIOLOGY, pediatric radiological case, March-April 2019
2. Cravo A C, Villacreses C, Silva J C. Osteopoiquilode: dois casos clínicos. ÓRGÃO OFICIAL DA SOCIEDADE PORTUGUESA DE REUMATOLOGIA - ACTA REUM PORT. 2006;31:255-60
3. Mahbouba J, Mondher G, Amira M, et al. Osteopoikilosis: A rare cause of bone pain. Caspian J Intern Med 2015; 6(3):177-9.
4. Pires Carvalho A C, Santos Beze R, Estevam Picinini S. Osteopoiquilose Apresentação de um caso e revisão da literatura. Radiol Bras 2002;35(3):1912
5. N. DAL PIZZOL, M.M. DAL PIZZOL. Osteopoiquilose: relato de caso. Rev Bras Ortop_Vol. 37, No 10 Outubro, 2002.

