A diabetic 63-year-old non smoker woman presented to the emergency department with an 8-day history of fever, shortness of breath and productive cough for which she had been treated with a 7-day course of clarithromycin without improvement. There were no previous complaints of respiratory or constitutional symptoms. Her physical examination was remarkable for an oxygen saturation of 93% while breathing room air, with no other signs of respiratory distress, and scant bilateral crackles and rhonchi were audible on pulmonary examination. Blood tests showed mild hypoxemia, leukocytosis and an elevated C-reactive protein. The chest X-ray depicted a well-defined round opacity with air bronchogram located in the upper segment of the left lower lobe (Figure 1 and 2). There were no signs of atelectasis or pleural effusion. A diagnosis of round pneumonia was presumed and she was started on amoxicillin-clavulanate. Blood cultures came positive for Streptococcus pneumoniae. One week later there was clinical and radiological improvement. Round pneumonia is classically associated with Streptococcus pneumoniae infections in pediatric patients. This pattern is thought to arise in children before 10 years old due to poor collateral ventilation in the presence of immature pores of Kohn and channels of Lambert.1 Most frequently the lesions appear as a single round opacity, variable in size, and with either smooth or slightly irregular borders. Lower lobes are the usual location, and air bronchogram is not a common feature.2,3 Potential agents also include Haemophilus influenzae, Coxiella burnetii and specific Legionella and Rickettsia species.3 This radiological presentation is very uncommon in adults, and the primary concern in differential diagnosis is malignancy, especially when antibiotic therapy does not lead to symptom resolution.2,3 Less frequently atelectasis, septic emboli, rheumatoid nodules and Granulomatosis with polyangiitis may present similarly.3 Awareness of this radiological pattern on adult patients is vital in order to avoid overtesting and overtreatment.
Figura I
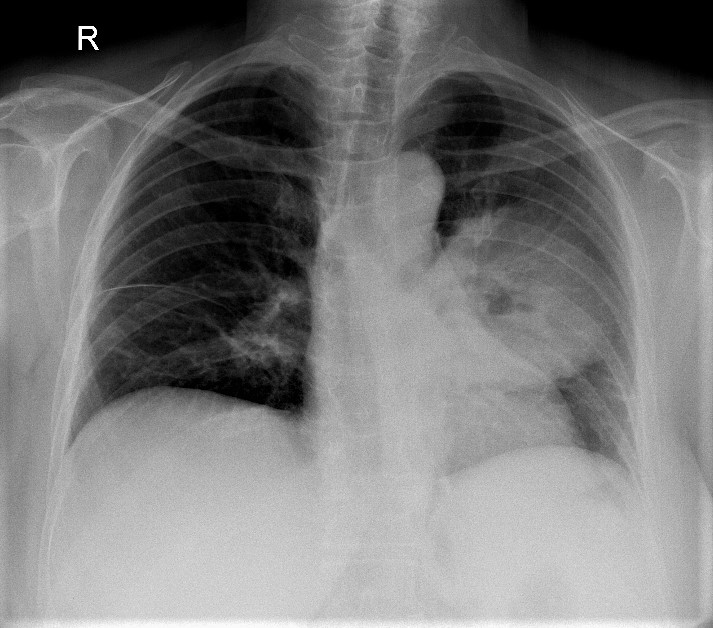
Posteroanterior chest radiography showing a well-defined round opacity on the left lung
Figura II
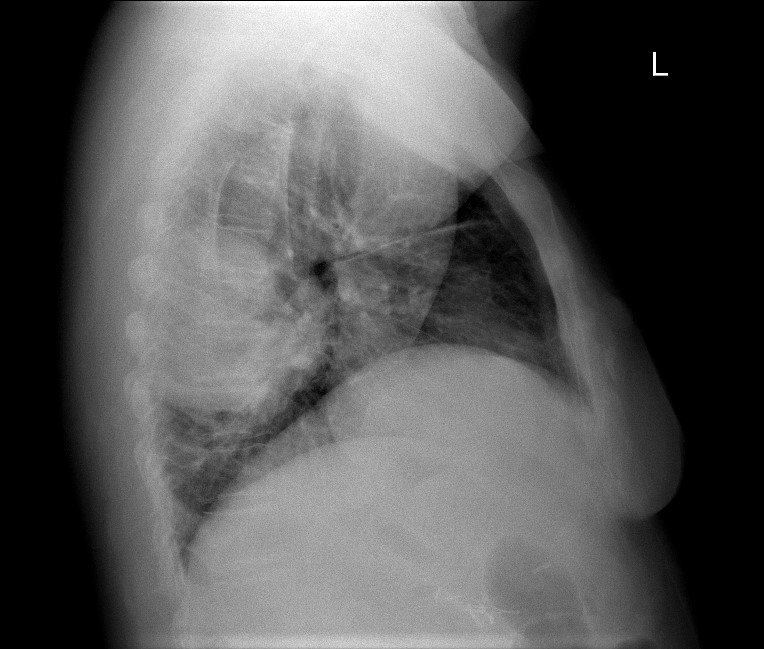
Left lateral view chest radiography showing a lesion on the left lower lobe
BIBLIOGRAFIA
1. Restrepo R, Palani R, Matapathi UM, Wu Y-Y. Imaging of round pneumonia and mimics in children. Pediatr Radiol. 2010;(40):193140. DOI: 10.1007/s00247-010-1767-7
2. Wagner AL, Szabunio M, Hazlett KS, Wagner SG. Radiologic manifestations of round pneumonia in adults. American Journal of Roentgenology. 1998;170(3):7236. DOI:10.2214/ajr.170.3.9490962
3. Cunha BA, Gran A, Simon J. Respiratory care. 2013; 58 (7): e80-e82. DOI: 10.4187/respcare.02219

