A neurocisticercose é a helmintíase mais comum do SNC.1, 2, 5 Causada pela Taenia solium, associa-se a consumo de carne de porco contaminada.4 É endémica em zonas com baixos recursos socioeconómicos sendo uma causa importante de convulsões mundial.3, 4 O diagnóstico é essencialmente imagiológico.4 A sequência de imagens corresponde a uma RMN craniana de uma senhora de 46 anos, cabo-verdiana, realizada em contexto de crise convulsiva tónico-clónica generalizada. As imagens A, B e C exemplificam lesão em fase vesicular nodular, observando-se na imagem B o escólex. Na D é envolvido do espaço subaracnoideu na vala sílvica à esquerda (seta branca) e a imagem E corresponde à fase nodular granular, já sem edema, onde se observa uma pequena lesão quística. A doente apresentava há mais de um ano cefaleias e hemiparestesias contralaterais. Este caso exemplifica o espetro de lesões na neurocisticercose, em diferentes fases de evolução, e com envolvimento de distintos compartimentos do SNC.4,5
Neurocysticercosis is the most common CNS helminthiasis.1,2,5 Caused by Taenia solium, it´s associated with consumption of contaminated pork.4 It´s endemic in areas with low socio-economic resources and is a major cause of seizures world wide.3,4 Diagnosis is essentially imaging4.The sequence of images corresponds to a cranial MRI of a 46-year-old Cape Verdean woman, performed in the context of a generalized tonic-clonic seizure. Images A, B and C exemplify a lesion in the nodular vesicular phase, with the scolex in image B. On image D, it´s invaded the subarachnoid space in the silvic ditch on the left (white arrow) and image E corresponds to the nodular granular phase, already without edema, where a small cystic lesion is observed. The patient had had contralateral headaches and hemiparesthesia for one year.This case exemplifies the spectrum of lesions in neurocysticercosis, in different stages of evolution, and involving different compartments of the CNS.4,5
Figura I
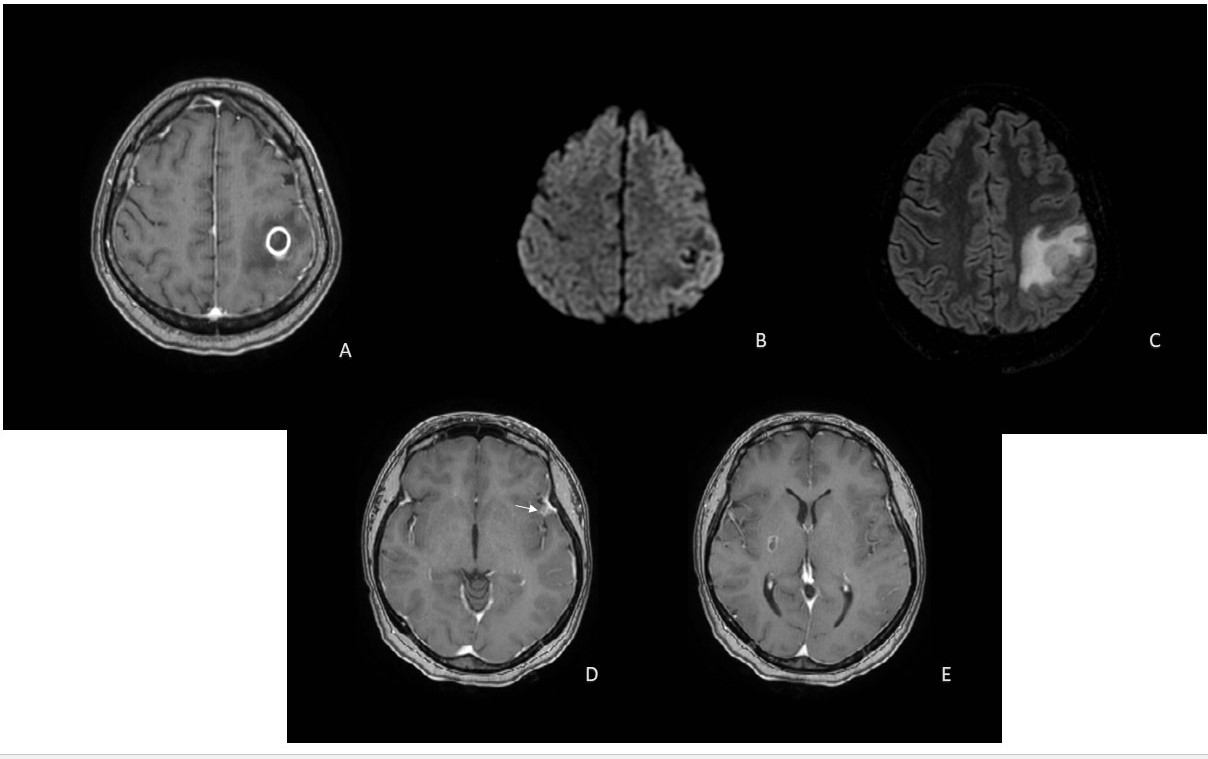
RMN do crânio
BIBLIOGRAFIA
1. White AC Jr et al. Diagnosis and Treatment of Neurocysticercosis: 2017 Clinical Practice Guidelines by the IDSA) and the ASTMH. Clin Infect Dis. 2018 Apr 3;66(8):e49-e75
2. Lucy B. Gripper, Susan C. Welburn. Neurocysticercosis infection and diseaseA review. Acta Trop. 2017 Feb;166:218-24.
3. Indar Kumar Sharawat, Renu Suthar. Calcified neurocysticercosis: The calcified dot is not so innocuous!. Seizure. 2020 Aug;80:65-6.
4. Santhosh AP, et al. Carbamazepine versus levetiracetam in epilepsy due to neurocysticercosis.Acta Neurol Scand. 2021 Mar;143(3):242-7.
5. Garcia HH, Nash TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. Lancet Neurol 2014; 13:1202

