A 54-year-old man with a recent diagnosis of hepatocellular carcinoma class C Barcelona-Clinic Liver Cancer (BCLC) Child Class B, presented to the emergency department with a 2-week history of fatigue and exertional dyspnea and non-productive cough. Physical examination was notable for hypertension (blood pressure, 155/90 mm Hg), tachypnea (28 breaths per minute), tachycardia (heart rate, 110 bpm), hypoxemia (oxygen saturation 90%, room air), holosystolic murmur, bilateral rales, upper right abdominal pain to palpation and hepatomegaly.
Computed tomography (CT) pulmonary angiography (Figure 1) showed multiple bilateral cannonball lesions, some converging into a pseudotumor-like aspect in the right lower lobe. Discrete peripheral pulmonary embolism, predominantly on the left side was also described, although not present on the static images.
A transthoracic echocardiography (Figure 2) showed biatrial enlargement (right larger than left). Inside the right atria there was a significant heterogeneous mass (34,4 mm x 34,6 mm) adherent to its roof, posterior wall and atrial septum, with several moving thread-like segments, without blood flow obstruction, and left ventricular hypertrophy with a normal function.
CT of the abdomen confirmed hematogenous dissemination of the hepatocellular carcinoma, which had no identifiable cleavage plane with the drainage point of the inferior vena cava (IVC) to the right atria.
The patients condition worsened after admission and he died.
Cannonball metastases are frequently seen in germ cell, renal, endometrial, prostate and gastrointestinal tumours. Only rarely are they due to hepatocellular carcinoma. Their presence often implies extensive disease dissemination and, therefore, a likely worse outcome.1,2
Extension of hepatocellular carcinoma to IVC and right atria is a rare complication, ranging from 1% to 4%, and is associated with pulmonary embolism and with a poor prognosis. 3,4
Figura I
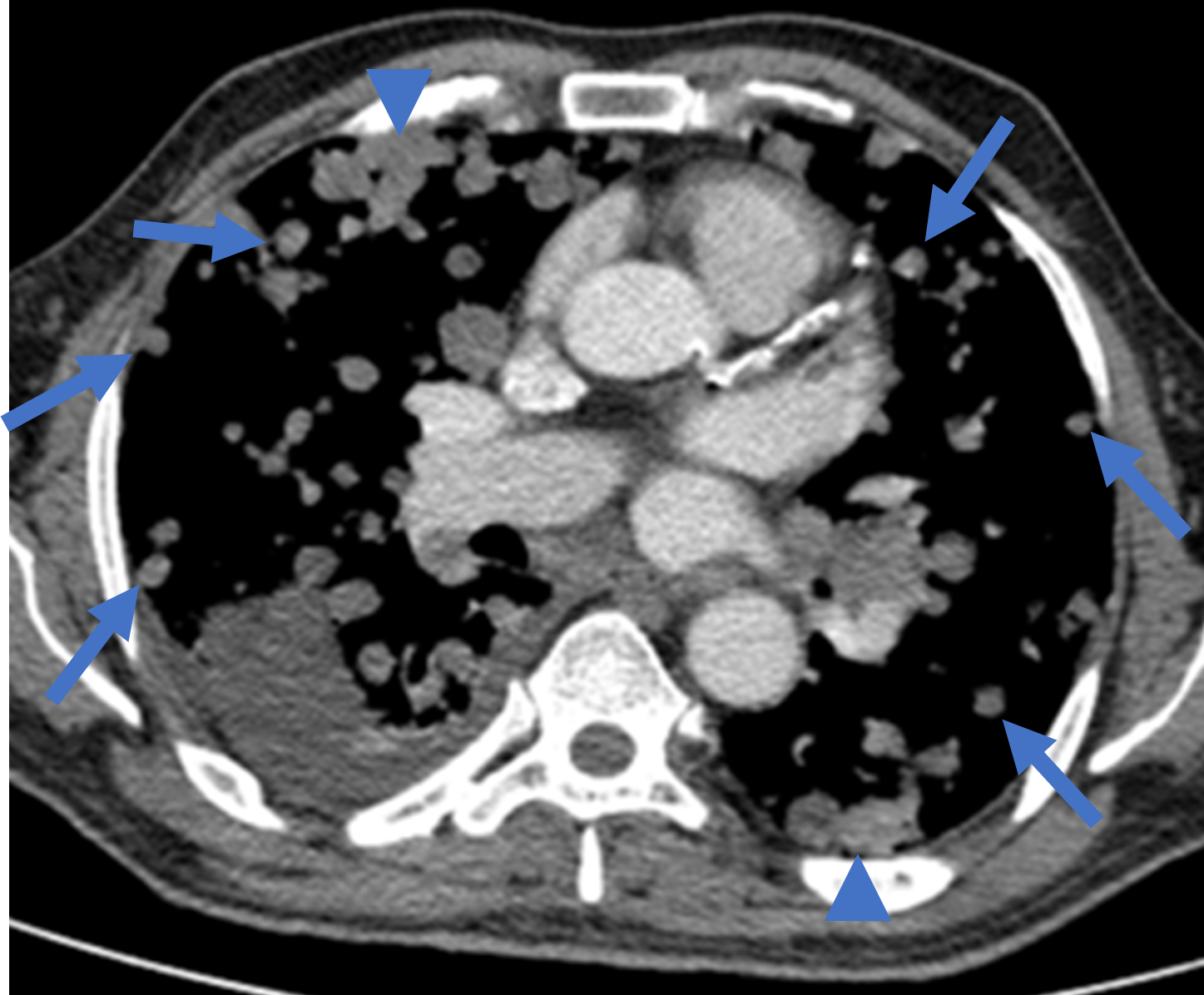
Computed tomography pulmonary angiography with multiple bilateral cannonball lesions (arrows), some confluent to form to form heterogenous mass-like opacities (arrowhead).
Figura II
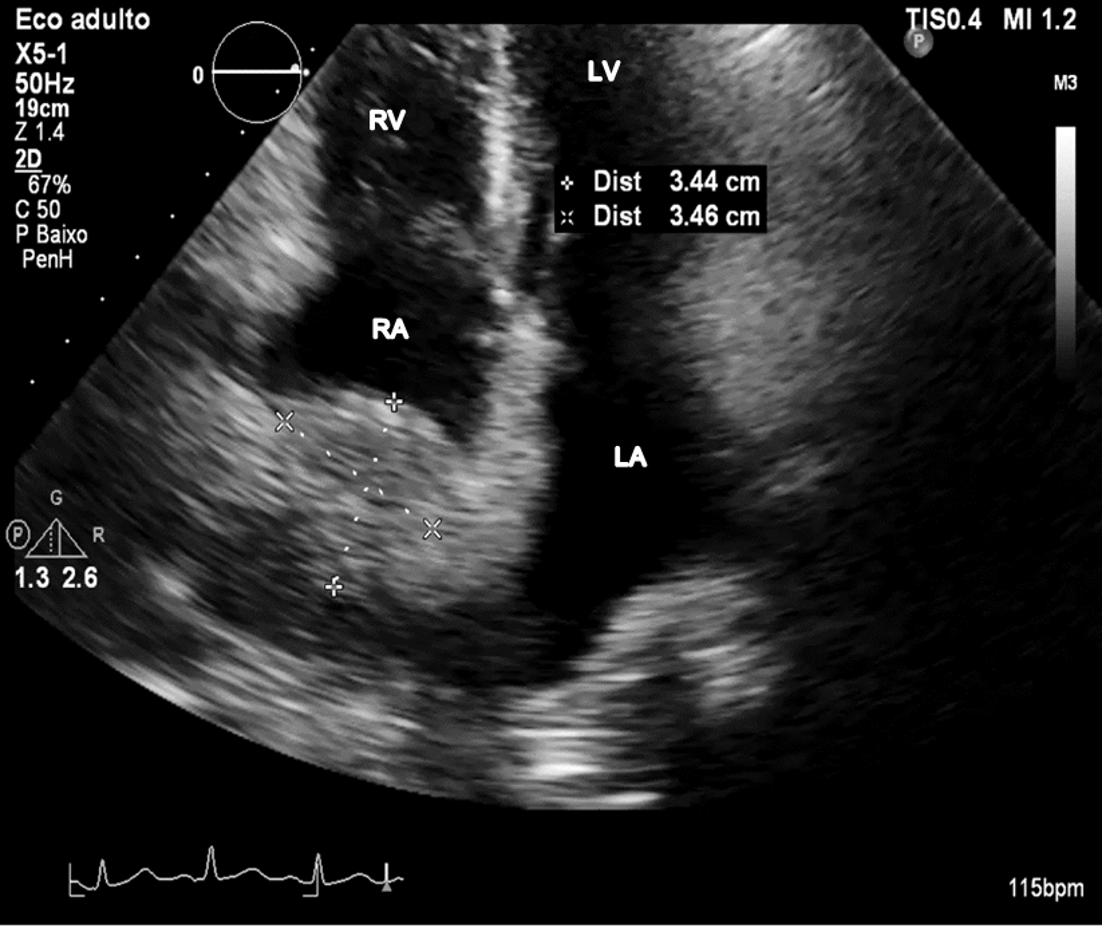
Transthoracic echocardiography with a right atrial mass. LA - left atrium, LV - left ventricle, RA - right atrium, RV - right ventricle
BIBLIOGRAFIA
1.Yang R-H, Ting C-H, Chu Y-K. Cannonball lung metastases as a presenting feature of ectopic hCG expression. J Oncol Sci. 2016 Aug; 2, 23: 5862. doi:10.1016/j.jons.2016.07.003
2. Chao, C. M., & Lai, C. C. Cannon ball pulmonary metastases. QJM: monthly journal of the Association of Physicians. 2015 Oct; 108(10), 843. doi.org/10.1093/qjmed/hcv097
3.Ohta M, Nakanishi C, Kawagishi N, Hara Y, Maida K, Kashiwadate T, et al. Surgical resection of recurrent extrahepatic hepatocellular carcinoma with tumor thrombus extending into the right atrium under cardiopulmonary bypass: a case report and review of the literature. Surg case reports. 2016 Dec; 2:110. doi:10.1186/s40792-016-0241-7.
4. Sundriyal, D., Bhargava, S., Sharma, N., & Gera, A. Cannon Ball Metastases and Atrial Thrombus. Indian journal of surgical oncology. 2015 Jun; 6(3), 311312. doi.org/10.1007/s13193-015-0426-8

