A 54-year-old man, with a tobacco, alcohol and cannabinoid abuse disorder, was admitted with a 3-month history of daily cough, more severe at night, sometimes with white sputum, that did not improve after therapy with desloratadine and acetylcysteine. The patient also had a 1-month history of two episodes of night sweats, and weight loss (9 Kg). He reported no fever nor past tuberculosis infection.
Upon physical examination, the patient presented crackles over the upper halves of both hemithoraces. Chest radiography (Fig. 1, A) revealed bilateral cavitary disease, and computed tomography (CT) of the chest (Fig. 1, Panel B) showed bilateral large cavities, mostly involving the upper lobes, as well as consolidation areas, dispersed nodules and lymphadenopathies of the mediastinum and hilum.
Sputum acid-fast bacilli (AFB) stain were consistently negative on several samples, but an AFB stain from bronchoalveolar lavage (BAL) was positive. Later, BAL and sputum cultures grewMycobacterium tuberculosis,susceptible to all anti-tuberculosis drugs. A test for human immunodeficiency virus was negative.
Quadruple standard therapy for tuberculosis was initiated and continued after discharge through directly observed treatment.
After three months of treatment, sputum cultures became negative; however, the patients condition deteriorated. Radiographic imaging (Fig. 1, C and D) worsened, with diffused consolidation on the upper left lobe, larger cavities with an air-fluid level, and scattered granulomas bilaterally. A new bronchoscopy excluded endobronchial lesions and stenosis, although a left tracheal deviation due to lung parenchymal traction was identified. BAL and sputum cultures were again negative for bacteria and mycobacteria.
A diagnosis of a paradoxical reaction to tuberculosis treatment was made; intensive therapy was extended for four months and then continuation therapy was kept for seven months, uneventfully and with a favourable progressive resolution of the lung lesions (Fig. 2, E and F).
Paradoxical reaction has been defined as the clinical or radiological deterioration of original tuberculous lesions or the emergence of new lesions in patients whose clinical condition initially improved with anti-tuberculosis treatment.1,2
When facing an apparent paradoxical reaction during tuberculosis treatment, it is essential to first exclude noncompliance, drug resistance, another secondary infection, and adverse drug effects.
Figura I
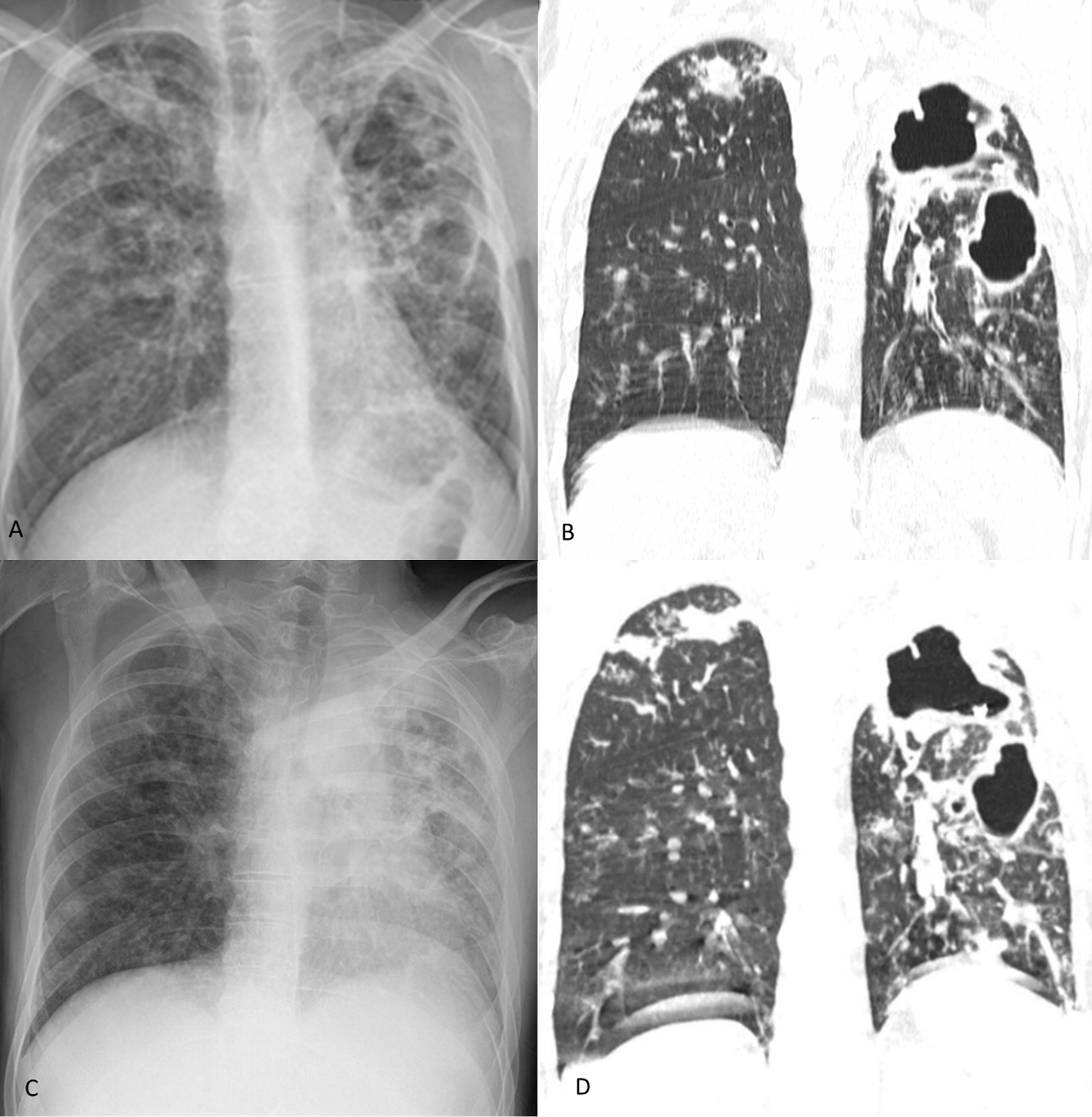
Patients radiographic imaging study on admission (A Chest radiography; B computed tomography of the chest) and upon paradoxical reaction (C Chest radiography; D computed tomography of the chest)
Figura II
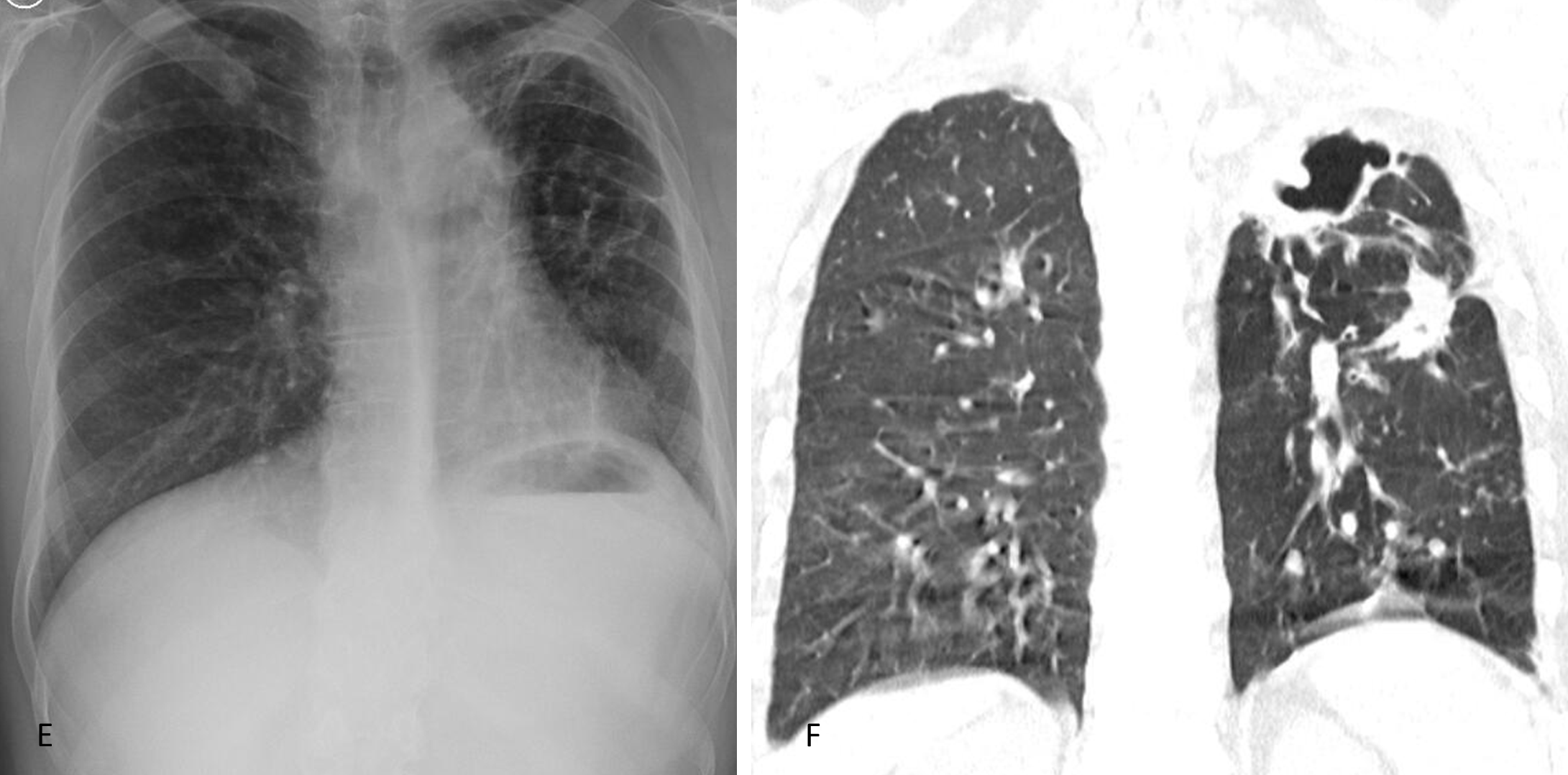
Patients radiographic imaging study two years after treatment (E Chest radiography; F computed tomography of the chest)
BIBLIOGRAFIA
1.Breen RAM, Smith CJ, Bettinson H, Dart S, Bannister B, Johnson MA, et al. Paradoxical reactions during tuberculosis treatment in patients with and without HIV co-infection. Thorax. 2004; 1;59:7047. doi: 10.1136/thx.2003.019224
2.Cheng VCC, Ho PL, Lee RA, Chan KS, Chan KK, Woo PCY, et al. Clinical spectrum of paradoxical deterioration during antituberculosis therapy in non HIV-infected patients. Eur J Clin Microbiol Infect Dis. 2002; 11:8039. doi: 10.1007/s10096-002-0821-2

